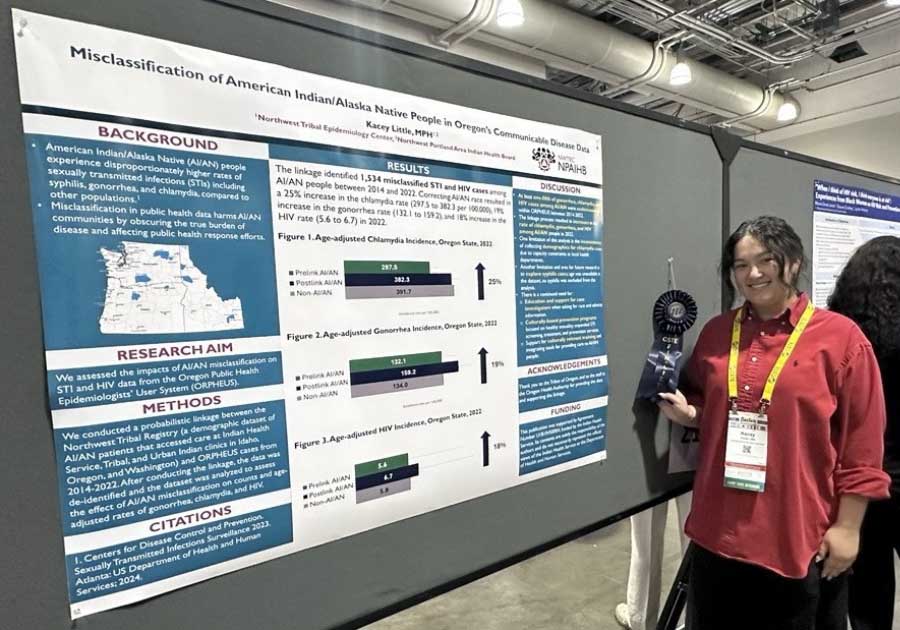
USET OTPH Opioid Recovery Series
In 2026, the USET Office of Tribal Public Health partnered with four Tribal Nations to elevate culturally grounded approaches to substance use recovery and healing through the USET OTPH Opioid Recovery Series. The series created a space for public health officials, counselors, psychiatrists, social workers, clinicians, service providers, clinical administration staff, and Tribal leaders to share strategies rooted in traditional knowledge and evidence-based practices.
The impact of the series so far is clear: 100% of participants who completed post-event surveys following January and April webinars reported that the trainings were a good use of their time. Participants described leaving the sessions with practical tools, renewed perspective, and deeper understanding of how recovery efforts can be strengthened through culture and community.
So far, the series has brought together 34 individuals representing 14 different Tribal Nations.
January Webinar: Physical Healing through Medication Assisted Treatment (January 29)
Presenters from the Catawba Nation shared how physical healing can be supported through Medication Assisted Treatment (MAT), an evidence-based approach that combines FDA-approved medications with counseling and behavioral therapies. The session aimed to provide a holistic perspective, grounded in traditional teachings and clinical best practices, to help participants better understand, implement, and support MAT in their Tribal Nations.
One participant reflected on the importance of broadening the conversation around recovery:
“I also left with a strong reminder that recovery is not an individual journey. Families and communities need support too — through grief support groups, craft groups, and community reinforcements — and through ongoing education that helps people better understand the medication and the disease, reduce stigma, avoid enabling, and learn how to walk alongside someone in recovery with care and awareness, without unintentionally becoming a trigger.”
April Webinar: Emotional Well-Being through Healing of the Canoe (April 30)
The Saint Regis Mohawk Tribe highlighted the role of emotional healing through Healing of the Canoe – a culturally grounded life skills and substance abuse prevention curriculum for Native youth. By sharing both traditional teachings and programmatic best practices, presenters equipped attendees with strategies to better understand, implement, and support prevention efforts within their own communities.
The session deeply resonated with participants, with one attendee sharing:
“Kids need and deserve an outlet to speak freely about substance abuse. This program is needed.”
Upcoming webinars in USET OTPH Opioid Recovery Series:
Building on the success of the first two sessions, the USET OTPH Opioid Recovery Series will continue to foster conversations that honor Tribal knowledge while addressing the complex realities of substance use recovery.
We invite TEC staff and your Tribal Nation partners to join us for the two remaining sessions in our Opioid Recovery Series. To register, click the links below.
June 25 – A Multi-Pronged Approach: The Role of Spirituality in Substance Use Recovery
8:30am Alaska / 9:30am Pacific / 10:30am Mountain / 11:30am Central / 12:30pm Eastern
Join us for an engaging session with Chief Spencer Lyons from the Onondaga Nation as they explore how spirituality can play an important role in substance use recovery. This session will share strategies on how to engage in meaningful conversations about spirituality and incorporate spirituality into substance use recovery programs.
August 26 – Whole Health: Strategies to Manage Co-Occurring Mental Health Disorders
8:30am Alaska / 9:30am Pacific / 10:30am Mountain / 11:30am Central / 12:30pm Eastern
Join us for an engaging session with the Tunica-Biloxi Tribe of Louisiana as they explore how substance use and mental health recovery can be supported through multi-disciplinary coordination. This session will share strategies to manage co-occurring mental health disorders in rural and tribal settings that often require coordination across departments, nuanced prescription management, and a team-first approach.
![]()